Pleural disease
•Download as PPTX, PDF•
3 likes•670 views

The document discusses pleural disease and pleural effusions. It covers pleural anatomy, physiology of pleural fluid formation and drainage, diagnostic evaluation of pleural effusions including physical exam, imaging like chest x-ray and CT, and diagnostic thoracentesis. Pleural effusions are classified as transudative or exudative. Common causes of exudative pleural effusions include infections like tuberculosis, malignancy, heart failure, and pulmonary embolism.
Report
Share




































































































































Pleural disease
- 1. Pleural disease
- 2. Outline Introduction Pleural anatomy Normal pleural fluid characteristic Pleural pressure and pleural manometry pleural effusion Classification and epidimiology Nonmalignant pleural effusion Pathophysiology Diagnostic approach Treatment Unclear exudate and idiopathic pleural effusion Malignant pleural effusion
- 6. The thoracic cavity is constructed like a vertical bellow Pleura and its space the pleural cavities are separated by the mediastinum, whereas other mammals (e.g., mice, American buffalo) lack complete separation between the left and right pleurae The adult elephant is the only mammal that does not possess a pleural cavity Introduction
- 7. The two pleural membranes meet at the hilar root of the lung In the sheep with a pleural anatomy similar to humans, the SA of the visceral pleura of one lung, including that invaginating into the lung fissures, is similar to that of the parietal pleura of one hemithorax approximately 1000 cm2 The normal pleural space is approximately 18 to 20 μm in width it widens at its most dependent areas It has been shown that the pleural membranes do not touch each other and that the pleural space is a real, not a potential
- 8. Anatomy of pleura • Pleura is a serous membrane covering the lung, mediastinum, diaphragm, and rib cage. • Divided into the visceral pleura covers the lung parenchyma including the interlobar fissures • Parietal pleura lines the inside of the thoracic cavities.
- 10. Embryology Developes from embryonic mesoderm Parietal and visceral pleura differentiate by the 3rd week of gestation Pleural cavity separate from pericardial cavity by 9th week of gestation Surface area (2000) cm² (adult male ) Pleural space (10-20 ) μm contain 8-10 ml of fluid Two layers joined at the pulmonary ligament
- 11. Blood supply The parietal pleura is supplied by inter costal arteries the visceral pleura is exclusively supplied by the bronchial circulation ,which drains into pulmonary veins. The drainage route via pulmonary veins may have contributed to earlier confusion about whether the visceral pleural blood supply was from a systemic (bronchial) or pulmonary circulation.
- 12. Lymphatic drainage If one injects carbon particles into the pleural space as a visible marker of lymphatic drainage pathways, one later finds that the black carbon has been taken up into lymphatics on the parietal side, not the visceral side The visceral pleura has extensive lymphatics, but they do not connect to the pleural space From the stomas, liquid drains to lacunae, spider-like submesothelial collecting lymphatics, which then drain to infracostal lymphatics, to parasternal and periaortic nodes, to the thoracic duct,and into the systemic venous system
- 13. Nerve supply The parietal pleura contains sensory nerve fibers, supplied by the intercostal and phrenic nerves, and has long been thought to be the major site of pain sensation in the pleura. The costal and peripheral diaphragmatic regions are innervated by the intercostal nerves, and pain from these regions is referred to the adjacent chest wall. The central diaphragmatic region is innervated by the phrenic nerve, and pain from this region is referred to the ipsilateral shoulder. The visceral pleura has more recently been shown to have sensory nerve fibers that may participate in pain or other sensations such as dyspnea.
- 14. Pleural fluid formation
- 15. The initial microvascular filtrate in the parietal and visceral pleura is partly reabsorbed. The remaining low-protein interstitial liquid flows across the leaky pleural mesothelial layers into the pleural space. The pleural liquid exits the pleural space via the parietal pleural lymphatic stomata.
- 16. Fluid can also enter the pleural space from intrestitial spaces of the lung via the visceral pleura or from peritoneal cavity through the small holes in diaphragm.
- 17. The entry rate of pleural liquid is approximately 0.01 mL/kg per hour , or about 0.5 mL hourly or 12 mL a day in a grown man. The majority of liquid exits the pleural space by bulk flow, not by diffusion or active transport. This is evident because the protein concentration of pleural effusions remains constant as the effusion is absorbed, as is expected with bulk flow. If liquid were absorbed by diffusion or active transport, proteins would exit at a slower rate and the protein concentration would progressively increase. The exit rate (0.28 mL/kg per hour) was nearly 30 times the baseline exit rate (0.01 mL/kg per hour).
- 18. Reliable data on the volume and cellular content of pleural fluid in normal humans are scarce because of the obvious difficulties in retrieving this small amount of fluid without “disturbing” the pleural environment.
- 20. Physiological Changes with Pleural Effusion When the pleural space is occupied by fluid, the pleural pressure becomes positive. The increase in volume must be compensated by an increase in the size of thoracic cavity or a decrease in size of the heart or lungs In experimental settings, the addition of saline in the pleural cavity causes 30% decrease in lung volume at functional residual capacity and 20% at total lung capacity
- 21. Physiological Changes with Pleural Effusion Therapeutic thoracocentesis has been shown to increase the FEV1 and FVC by 200 ml for every 1000 ml removed fluid. The increase in maximal inspiratory pressures post thoracocentesis, is greater than the improvement in lung volume; relief of the downward displacement of the diaphragm is probably responsible for this finding. Pleural effusion leads to an ipsilateral intra-pulmonary shunt, which does not significantly change after thoracocentesis. Consequently, PaO2 does not increase after thoracocentesis, may actually decrease paradoxically.
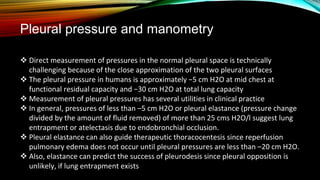
- 22. Pleural pressure and manometry Direct measurement of pressures in the normal pleural space is technically challenging because of the close approximation of the two pleural surfaces The pleural pressure in humans is approximately −5 cm H2O at mid chest at functional residual capacity and −30 cm H2O at total lung capacity Measurement of pleural pressures has several utilities in clinical practice In general, pressures of less than –5 cm H2O or pleural elastance (pressure change divided by the amount of fluid removed) of more than 25 cms H2O/l suggest lung entrapment or atelectasis due to endobronchial occlusion. Pleural elastance can also guide therapeutic thoracocentesis since reperfusion pulmonary edema does not occur until pleural pressures are less than –20 cm H2O. Also, elastance can predict the success of pleurodesis since pleural opposition is unlikely, if lung entrapment exists
- 23. Digital pleural manometer
- 24. Lung entrapment and entrapped lung Lung entrapment is a term given to non-expandable lung due to active pleural inflammation, malignancy, or haemothorax. The term is similar but not entirely synonymous with trapped lung, which is due to pleural inflammation from remote disease resulting in fibrous thickening of the pleura.
- 25. pPr is slightly ve and as fluid is withdrawn, it comes down which suggests that lung is expanding and returning to its normal position top tracing. entrapped lung,initial pPr ve and the first part of the curve behaves like a normal lung but later, pPr falls quickly. This is suggestive of entrapped phase and denotes that lung will not be able to expand further . trapped, the curve is monophasic,initial pPr is already -ve and falls quickly , bottom , suggests unexpanded lung and indicates that pleurodesis is likely to fail in this situation, as the basic principle of pleurodesis is that both visceral and parietal pleurae have to oppose each other to obtain a successful pleurodesis.
- 27. recap the pleura is a serosal membrane which functions to reduce the friction during lung movement. Normal pleural fluid is a microvascular filtrate formed from the parietal pleural capillaries, predominantly drained via the lymphatic stoma. Pleural manometry increasingly used to diagnose trapped lung, predict success of pleurodesis and guide therapeutic thoracocentesis.
- 28. A 45-y-F present with a 3-week history of mild SOB. not drink or smoke. in good health until she began losing weight 2 months ago. FHX is unremarkable. She is afebrile, chest reveals dullness and decreased breath sounds at the left base. Her abdomen is not tender and has normal bowel sounds. The results of laboratory studies and her chest radiograph are shown below. ThoracentecisPeriphral blood Cells per μL 980Haematocrit % 37 Lymphocytes % 70 Neutrophils %20 Mesothelial cells % 1 Pleural fluid pH 7.37 Leukocytes per μL 8700 Neutrophils % 67 Lymphocytes %20 Monocytes % 10 Eosinophils % 3 Protein g⋅L−1 4.3Serum protein g⋅L−1 6.2 Glucose mmol⋅L−1 3.4 Serum lactate dehydrogenase U⋅L−1 300 Glucose mmol⋅L−1 3.9 Serum lactate dehydrogenase U⋅L−1 210 Cytology No malignant cells
- 30. Which of the following is the most likely explanation for the effusion? a. Small oesophageal rupture b. Pancreatitis c. Meigs’ syndrome d. Mesothelioma e. Tuberculous pleurisy
- 31. Which of the following is the most likely explanation for the effusion? a. Small oesophageal rupture b. Pancreatitis c. Meigs’ syndrome d. Mesothelioma e. Tuberculous pleurisy
- 32. Pleural effusion Pleural effusion, the accumulation of fluid in the pleural cavity, is a common clinical problem encountered in general practice.
- 33. CLASSIFICATION - Pleural effusion→classif. Non malignant PE Malignant PE
- 34. CLASSIFICATION - Pleural effusion→classif. TRANSUDATE PE EXUDATE PE
- 35. For pleural liquid to accumulate to form an effusion, it is likely that both the entry rate of liquid must increase and the exit rate must decrease. If only the entry rate increased, it would require a sustained rate more than 30 times normal to exceed the reserve lymphatic removal capacity; if the exit rate decreased, it would take more than a month at the normal entry rate of 12 mL per day to produce an effusion detectable by chest radiograph. Thus, in the clinical setting, it is most likely that excess pleural liquid accumulates due to changes in both entry and exit rates.
- 36. • Pleural fluid (PF) collects by one or more mechanisms: (1) pleural injury that causes increased pleural membrane permeability and protein-rich exudates (2) increased intravascular hydrostatic forces and/or decreased oncotic forces that cause protein-poor transudates (3) extravasation of fluid from lymphatic or vascular structures or from an adjacent body compartment into the pleural space
- 41. MASSIVE EFFUSION 1-TB 2-Empyema 3-hepatic hydrothorax 4-chulo. 5-hemoth. 6-CHF 7-Malignant effusion
- 42. Approach to pleural effusion HISTORY the most com .is dyspnea, chest pain, cough and haemotysise Dyspnea due to pleural effusion is multifactorial and due to lung compression, decreased compliance of the chest wall, and depression of the diaphragm. Chest pain may be caused by the presence of pleural fluid itself or be due to the underlying pathology responsible for the effusion cough is not specific, characteristics of the cough may aid identification of the underlying cause hemoptysis suggest that the effusion. lung cancer, pulmonary embolism, or tuberculosis
- 43. Weight loss ------ Night sweats should prompt investigations-------- Joint, skin, or eye disease may indicate------ Orthopnea, PND, peri. edema, and DET ------- drug history should be taken to evaluate this possibility amiodarone,clozapine,ergots, methotrexate, nitrofurantoin, thiazolidinediones,multiple antineoplastic agents, and illicit drugs occupational history specfically seeking information regarding exposure to asbestos A social history smoking, excess alcohol intake
- 44. Physical examinasion Sign of effusion -------- only detectable when >250–300 cm3 of pleural fluid is present <300 ml → not detectable on clinical examination 500 ml → dull percution note ,decrease breath sound ,decrease fremitus >1000 ml →bulging of ICS ,decrease chest expansion ,bronchovesicular sounds and egophony at upper level of effusion
- 45. Physical examinasion Finger clubbing and Horner’s-------- ca bron. jaundice and ascites --------hepatic hydrothorax; Extensive lymphadenopathy and splenomegaly point toward lymphoma; a harsh ejection systolic murmur, slow rising pulse, and pedal edema --- CHF due to AS swollen, tender calf and loud second heart sound raise the prospect of pulmonary embolism
- 46. INITIAL DIAGNOSTIC TESTS CXR 5 ml → blunting of PCP angle on LD film 50-75 ml → blunting of PCP angle on L view 175-200 ml → blunting of PCP angle on PA view. > 500 ml → opacification of lung base
- 47. ULTRASOUND has a role both in image guidance for thoracentesis and chest drain insertion in local anesthetic thoracoscopy/pleuroscopy, provides valuable diagnostic information at the bedside. is superior to chest radiography in the identification and quantification of pleural effusions. In addition, it may show features specific for malignancy, such as visceral and parietal pleural thickening and diaphragmatic nodules or thickening. Ultrasound is more sensitive than CT in the detection of septations in patients with parapneumonic effusions.
- 48. C-CT performed in the presence of pleural fluid is of value in evaluating the cause of pleural effusion. Pleural nodularity, irregularity, circumferential pleural thickening, pleural thickening involving the mediastinal surface or thickening >1 cm are specific features of malignant pleural disease. CT performed prior to complete drainage of pleural fluid provides reliable identification of features of malignancy. Pulmonary embolism may be diagnosed with CT.
- 49. CT scan CT may demonstrate signs of asbestos exposure such as folded lung, pleural thickening, and pleural plaques, indicating the potential for the effusion to be related to asbestos. In the case of malignancy, CT will, particularly if the abdomen and pelvis are included, provide information needed to stage cancer, or identify a primary site in the case of metastatic disease to the pleura.
- 50. POSITRON EMISSION TOMOGRAPHY-CT positron emission tomography-CT (PET-CT) has shown promise in the investigation of inpatients with pleural effusions. Uptake is also elevated, however, in patients for years following talc pleurodesis and in patients with pleural infection. Currently, PET-CT does not have a role in the routine investigation of pleural disease, though it may have a role in monitoring response to treatment in mesothelioma.
- 51. MAGNETIC RESONANCE IMAGING MRI may represent an alternative imaging modality in patients in whom contrast is contraindicated for reasons of renal impairment or allergy. MRI has also been studied in its role for monitoring treatment response in mesothelioma
- 52. PLEURAL FLUID ANALYSIS Virtually all patients with a newly discovered pleural effusion should undergo thoracentesis to assist in diagnosis and management. Exceptions include a clear clinical diagnosis, such as typical CHF or a very small pleural effusion in a patient with presumed viral pleurisy. Observation is warranted in such cases; however, if the clinical situation worsens or is atypical, thoracentesis should be performed without delay. For example, if the patient with CHF has pleuritic chest pain, fever, unilateral pleural effusion, or oxygen tension out of proportion to the clinical situation, thoracentesis should be performed promptly.
- 53. Prospective study of 129 patient(1987) PFA ---------Diagnostic in 18% PFA----------presumptive diagnosis in 55% PFA----------NOT DIAGNOSTIC IN 27% 30 ML of fluid needed
- 54. PLEURAL FLUID ANALYSIS
- 55. Intercostal arterial anatomy at enhanced chest CT. A and B, Sagittal enhanced chest CT medially (A) shows the presence of the intercostal arteries positioned in the middle of the intercostal space (arrows, A), compared with the position along the inferior margin of the rib more laterally (arrow, B). C, Coronal maximum intensity projected enhanced CT image shows the courses of the intercostal arteries, positioned in the middle of the intercostal space medially (arrowheads) and along the inferior margin of the rib more laterally (arrows). (Courtesy Michael Gotway, MD.) A B C → → → → A B C <
- 56. If the pleural effusion is likely to be a transudate with low protein and lactate dehydrogenase (LDH) levels, the diagnostic possibilities are limited and are often easily discernible from the patient’s clinical presentation. Most transudates are due to CHF with the next most common (but much less frequent) cause being hepatic hydrothorax. By contrast, an exudative effusion has a far larger number of possible causes and in many cases poses a greater diagnostic challenge
- 58. Between 1% and 10% of malignant pleural effusions may be characterized as transudates by Light’s criteria pleural effusions due to heart failure may be classified as exudates in around 27% of cases, an effect that is exaggerated by prior diuretic therapy
- 59. Recommended initial pleural fluid assays RationalAssay To distinguish transudates from exudates Peritoneal dialysis, CVC erosion, duropleural fistula TB pleurisy Bacterial empyema, paragonimiasis, amebic empyema, septic emboli, rheumatoid pleurisy Protein and LDH <1 g/dL >4 g/dL LDH >1000 IU/L To identify pleural infection and other conditions causing low pHpH To identify pleural infection and other conditions causing low pleural fluid glucose Glucose To identify malignant cellsCytology: distinguish lymphocytic, eosinophilic, and neutrophilic effusionsDifferential cell count + Abnormal cells To identify intrapleural infection, the causative organism, andMicrobiology: Gram
- 60. Complicated parapneumonic effusion, chronic rheumatoid pleurisy, paragonimiasis, amebic empyema, esophageal rupture, TB pleurisy, lupus pleuritis Urinothorax Peritoneal dialysis, CVC erosion Glucose PF/S < 0.5 PF /S >1 Esophageal rupture, chronic rheumatoid pleurisy, complicated parapneumonic effusion, paragonimiasis, amebic empyema, TB pleurisy, lupus pleuritis, urinothorax, pancreaticopleural fistula PH <7.3
- 61. Cell count and difrential HemothoraxPF/S HCT>50RBC Parapneumonic effusion, lupus pleuritis, acute pancreatitis Empyema Ne.>10000 Ne.>50000 neutrophil TB pleurisy, sarcoid, chronic rheumatoid pleurisy, yellow nail syndrome, chylothorax 85-95lymphocyte Hemothorax, pneumothorax, benign asbestos pleurisy, pulmonary infarction, coccidioidomycosis, paragonimiasis and other parasites, drug-induced pleurisy, duropleural fistula, Churg–Strauss syndrome, sarcoidosis, TB pleurisy Eos.>10eosinophil Predominant in transudate,variable number in exudate Usually absent in paraneumonic and Tuberculous effusion Mesothelial cell
- 62. Pleural liquid that is submitted for white cell count and differential should be sent in a tube with an anticoagulant to prevent the cells from clumping. A pleural fluid white blood cell count of 1000/μL roughly separates transudative from exudative pleural effusion. the etiologies of 392 cases of eosinophilic pleural effusions have been reported as follows: idiopathic 40%, malignancy 17%, parapneumonic 13%, tuberculosis 6%, PE 4%, transudates 8%, and other 13%.
- 63. Specialized pleural fluid assays RationaleSpecialized assay Evaluation of heart failure as a cause of pleural effusion where diagnosis is unclearNT-pro-BNP (Blood or pleural fluid) Identification of effusions due to pancreatic pathology (not specific without isoenzyme analysis) and esophageal rupture Amylase (± isoenzyme analysis) Chylothorax, CVC erosion if lipids infused Cholesterol effusion(pseudochylothorax) TG >110 mg/dL Cholest.> 200 mg/dL ChylothoraxChylomicron URINOTHORAXCrea.PF/S>1 Biliopleural fistula Duropleural fistula, ventriculoperitoneal shunt migration Blirubin PF/S>1 Beta 2 transferrin tuberculous pleural effusionADA>40 mg/dl
- 64. Diagnoses that can be established definitively by pleural fluid analysis Diagnostic testsDiagnosis Cytological evidence of malignancyPleural malignancy Effusion Pleural fluid appearance (pus) and positive microbiological cultureEmpyema/parapneumonic Positive acid-fast bacilli stain, mycobacterial cultureTuberculous pleural effusion Positive fungal stain or fungal cultureFungal pleurisy Triglycerides >110 mg/dL, chylomicronsChylothorax Cholesterol >200 mg/dL, cholesterol crystalsPseudochylothorax Acidic pleural fluid, food contents within pleural fluidEsophageal rupture
- 65. Diagnoses that can be established definitively by pleural fluid analysis Diagnostic testsDiagnosis Hematocrit (pleural fluid/blood ratio >0.5)Hemothorax Pancreatic isoenzyme amylase(pleural fluid/blood ratio >1 or pleural fluid > normal serum reference range) Effusion due to pancreatitis Pleural fluid results consistent with dialysate used (protein <1 g/dL, glucose >300 mg/dL)Peritoneal dialysis Creatinine (pleural fluid/blood ratio >1)Urinothorax
- 66. Complications from thoracentesis pneumothorax and hemothorax Estimates of each complication from prospective studies are low (2% to 6% for pneumothorax; 1% for hemothorax)
- 67. TIME TO RESOLUTION Knowledge of the time of resolution, either spontaneous or with therapy, of pleural effusions can be helpful diagnostically. For example, an effusion from a pulmonary embolism rarely persists for more than 1 month benign asbestos pleural effusion may not resolve for 1–12 months tuberculous pleural effusions resolve over 1–4 months effusions from yellow nail syndrome and trapped lung are persistent.
- 68. 68 Y M pres. With PEF on abdominal imaging before 1 wk PMHX .stage2B AD pancreas. history of hypertension, diabetes mellitus, and chronic kidney disease (CKD) stage 5 with a baseline serum creatinine level of approximately 3.5 mg/dL and an (EGFR) of 15 mL/min/1.73 m2. PSHX distal pancreatectomy and splenectomy 6M agoو He has completed adjuvant chemotherapy and radiation, He requires hemodialysis transiently in the postoperative period and is now receiving furosemide O/EX. Emciated ,jvp not elevated,cardic ex.unremarkable
- 69. Lab. serum cr 4.1 mg/dL glucose 225 mg/dL albumin 2.5 g/dL lactate dehydrogenase (LDH) 166 U/L total protein ( P) 7.3 g/dL. Recent echocardiography are reviewed and are notable for left ventricular hypertrophy with impaired relaxation.
- 70. Pleural fluid Parameter Result Appearance Clear yellow pH 7.42 Leukocyte count 600/μL (65% neutrophils) Glucose 203 mg/dL LDH 220 U/L TP 3.1 mg/dL Cholesterol 41 mg/dL Amylase 16 U/L Cytology Negative
- 72. Which o the following is most accurate about the nature of this patient’s pleural effusion ? A. It is classified as a transudate by Light’s criteria. B. It is a discordant exudate by Light’s criteria. C. It is the result of esophageal rupture. D. It is the result of pancreatic inflammation. E. Repeat pleural cytology is likely to be positive.
- 73. B. It is a discordant exudate by Light’s criteria.
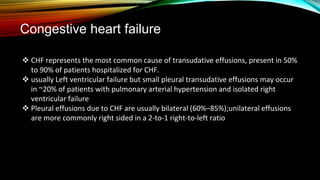
- 74. Congestive heart failure CHF represents the most common cause of transudative effusions, present in 50% to 90% of patients hospitalized for CHF. usually Left ventricular failure but small pleural transudative effusions may occur in ~20% of patients with pulmonary arterial hypertension and isolated right ventricular failure Pleural effusions due to CHF are usually bilateral (60%–85%);unilateral effusions are more commonly right sided in a 2-to-1 right-to-left ratio
- 75. CHF ------TRAN. But in 30%-----exudate its called psudoexudate Its explained by 1-use of diuretic 2-coexestance cause of exudate 3-some CHF-related effusions have PF erythrocyte count >10,000/μL, which causes sufficient release of LDH from red cell autolysis to fulfill Light’s criteria for an exudate.
- 76. Question 2: Which of the following additional tests on this patient’s pleural fluid would be most helpful in confirming the etiology of his effusion? A. Albumin level B. triglyceride level C. Adenosine deaminase level D. Flow cytometry E. Fungal cultures
- 77. Question 2: Which of the following additional tests on this patient’s pleural fluid would be most helpful in confirming the etiology of his effusion? A. Albumin level B. triglyceride level C. Adenosine deaminase level D. Flow cytometry E. Fungal cultures
- 78. When faced with the discordant exudate by Light’s criteria in a patient clinically suspected of having a transudate, the most immediate option available to the physician is the calculation of the serum-pleural protein gradient The transudative nature of the pleural fluids can be established in pseudoexudate by : if the serum minus the pleural fluid protein level is greater than 3.1 g/dL(62%) the serum minus the pleural fluid albumin level is greater than 1.2 g/dL.(correctly reclassifiying > 80%)
- 79. Question 3: Which of the following is the most accurate description of the principal mechanism of the accumulation of pleural fluid in this patient? A. Decreased fluid drainage due to obstruction of pleural lymphatics B. Increased pleural capillary permeability C. Reduced pleural capillary oncotic pressure D. Reduced central venous pressure E. Increased pulmonary capillary hydrostatic pressure
- 80. Question 3: Which of the following is the most accurate description of the principal mechanism of the accumulation of pleural fluid in this patient? A. Decreased fluid drainage due to obstruction of pleural lymphatics B. Increased pleural capillary permeability C. Reduced pleural capillary oncotic pressure D. Reduced central venous pressure E. Increased pulmonary capillary hydrostatic pressure
- 81. Question 4: Which of the following is true about N-terminal pro-brain natriuretic peptide (NT-proBNP) measurements in the evaluation of pleural effusions in the setting of heart failure? A. NT-proBNP is cleared by the liver and thus its levels need to be interpreted with caution in advanced hepatic disease. B. Pleural and serum NT-proBNP levels are elevated only in congestive heart failure with reduced ejection fraction. C. Serum NT-proBNP levels are highly correlated with those of pleural fluid in a given patient. D. Pleural NT-proBNP is inferior to the serum-pleural protein gradient in correctly classifiying discordant exudates identified by Light’s criteria. E. The high negative predictive value of clinical signs of heart failure obviates the need for NT-proBNP measurement in their absence when evaluating pleural effusions.
- 82. C. Serum N -proBNP levels are highly correlated with those of pleural fluid in a given patient.
- 83. Brain natriuretic peptides comprise a family of neurohormones released by cardiac myocytes in response to increased ventricular filling pressures as may be seen in the setting of systolic or diastolic left ventricular dysfunction. NT-proBNP and its cleavage product, BNP, are both renally cleared, which can affect their utility in advanced kidney disease. The accuracy of pleural fluid NT-proBNP in discriminating between effusions caused by heart failure and those that are not .exceeding 90% and is superior to that of BNP.
- 84. Although measurement of these peptides in pleural fluid is not widely available, studies have demonstrated such an excellent correlation between pleural and serum levels that serum testing can be substituted without sacrificing performance characteristics. Additionally, pleural fluid NT-proBNP is similar to the albumin gradient and superior to the protein gradient in the ability to correctly identifiey cardiac effusions misclassified as exudates by Light’s criteria. The physical examination in heart failure is not suficiently sensitive to obviate biochemical testing in cases of suspected cardiac effusion, though normal cardiac size on the chest x-ray is inconsistent with that diagnosis.
- 85. Rules for Evaluating Heart Failure– Related Effusions Misclassified as Exudates More accurate than protein or albumin-based testing rulesSerum amino terminal fragment of proBNP(NT-proBNP) >1500 pg/mL CHF-related <400 pg/mL CHF-unrelated High accuracy but no advantage over serum NT-proBNPPleural fluid assay of NT-proBNP >1500 pg/mL CHF-related <400 pg/mL CHF-unrelated Lower discriminative properties as compared with NT-proBNPPleural fluid BNP >400 pg/mL CHF-related <100 pg/mL CHF-unrelated
- 86. Treatment Patients with CHF and pleural effusion should be treated with afterload reduction, diuretics, and inotropes as needed. If the patient is markedly dyspneic when first evaluated, a therapeutic thoracentesis to relieve the dyspnea should be considered. Rarely, despite intensive therapy of the CHF, a patient has persistent large effusions; if such patients are dyspneic and if their dyspnea is relieved by a therapeutic thoracentesis, consideration can be given to controlling the effusions with a pleurodesis using a sclerosing agent, such as doxycycline or talc slurry, or the insertion of an indwelling catheter.
- 87. Parapneumonic Effusions Twenty to 57% of patients hospitalized for community-acquired pneumonia develop a parapneumonic effusion, as defined by a pleural effusion caused by pneumonia
- 88. 69 Y M 5 Days prod.cough fever rigor PMHX –VE ON/EX: PR 104 , RR 22, SPO2 95 with 2 l/m oxygen, lung exam .↓breath sound and in LL chest,dull percusion without egophony LAB Wbc 26000, (LDH) 139 U/L ,ser TP 6.6 g/dL , FBS 81 g/dL
- 89. Pleural fluid Parameter Result Appearance Clear yellow Cell count 660 cells/μL with 88% neutrophils pH 7.08 LDH 1,249 U/L total protein 4.6 g/dL Glucose 25 g/dL Gram stain Gram+ cocci in pairs and chains
- 91. Q 1: Which of the following options correctly pairs the most appropriate terminology to describe this patient’s pleural effusion with an appropriate single management strategy? terminology Management A Simple parapneumonic E Thoracotomy B Simple parapneumonice E Video-assisted thoracoscopic surgery(VATS) C Complicated parapneumonic E Antibiotics D Complicated parapneumonic E VATS E Empyema Thoracotomy
- 92. terminology Management A Simple parapneumonic E Thoracotomy B Simple parapneumonice E Video-assisted thoracoscopic surgery C Complicated parapneumonic E Antibiotics D Complicated parapneumonic E VATS E Empyema Thoracotomy
- 93. Classification simple parapneumonic E: sterile, free- flowing fluid generated by increased pleural capillary permeability needs AB & no drainage complicated parapneumonic E: extension of the infection into the pleural space with possible fluid loculation. mandate drainage in addition to AB Empyema: frank pleural pus .
- 94. Parameter Simple Complicated Empyema Appearance Clear Clear or cloudy Pus pH > 7.20 < 7.20 Not required LDH < 1,000 U/L > 1,000 U/L Not required Glucose > 40 mg/dL < 40 mg/dL Not required Microbiology -ve + /–Gram stain/culture + /–Gram stain/culture Management AB AB+ drainage AB+ drainage Modifed from the work of Davies et al.16 and Heffner et al.17
- 95. This patient’s effusion is classified as a CPE based on the pH, LDH, and positive Gram stain. The ACCP guidelines also consider fluid loculation as a criterion or labeling a parapneumonic effusion as complicated. In current practice, both image-guided tube thoracostomy as well as VATS are viewed as appropriate initial drainage options For CPE.
- 96. Empyemas require immediate evacuation, which will usually be accomplished via VATS, but a trial of chest tube drainage can be attempted, especially in poor operative candidates
- 97. Q 2: Which o the following procedural factors is most likely to reduce the risk of iatrogenic pneumothorax during the performance of this patient’s initial thoracentesis? A. Diagnostic versus therapeutic procedure B. Greater operator experience C. The use of real-time ultrasound guidance D. Lower number of needle passes E. Initial versus repeat procedure
- 98. only real-time sonographic guidance is unequivocally associated with a reduced risk of iatrogenic pneumothorax. C. The use of real-time ultrasound guidance
- 99. Q 3: Which of the following advantages can be expected from the insertion of a small-bore (i.e., 14Fr) chest tube rather than a large-bore (i.e., 32Fr) chest tube for the drainage of the infected pleural space? A. Reduced hospital stay B. Reduced pain upon insertion C. Reduced mortality at 1 year D. Reduced need or surgery at 1 year E. Reduced radiographic abnormality at 3 months
- 100. B. Reduced pain upon insertion
- 101. Malignant Pleural Effusions It means presence of malignant cells in pleural space 15% of patient who died with cancer Malignant pleural effusions (MPE) constitute the second most common cause of exudative pleural effusions in the developing country. It is increasingly recognized that malignant cells can reach the pleural space without effusion because lavage of the pleural space before resection of lung cancer in those without effusion can have positive cytologic results Its most common cause of lymphocytic effusion
- 102. In one study of more than 1200 patients with lung cancer without effusion undergoing curative surgical resection, 5.3% had positive pleural cytologic findings on lavage at the time of thoracotomy before resection
- 103. The diagnosis of pleural malignancy is the first indication of cancer in about 10% of effusions. Primary pleural malignancy is an uncommon cause of malignant pleural effusion and metastatic malignant pleural effusions are 25-fold common than mesotheliomas even in areas where the latter are relatively common.
- 104. ETIOLOGY OF MALIGNANT EFFUSIONS Total (%)Primary Tumor Site 37.5Lung 16.8Breast 11.5Lymphoma 6.9Gastrointestinal 9.4Genitourinary 7.3Other 10.7Unknown
- 105. Lung cancer Pleural effusions are present in 15% of patients of lung cancer at diagnosis 50% of patients develop effusion during their disease course adenocarcinomas are most frequently associated with malignant pleural effusions, but effusions may be seen with all types
- 106. Carcinoma of breast Breast cancer is the second most common cause, the time from the initial diagnosis to development of effusion is usually two years, but can extend up to 20 years. effusion usually is ipsilateral to the site of the original tumor (50%) but can also be contralateral (40%) and less commonly bilateral (10%).
- 107. Lymphoma the 3rd most common cause in most series, but is possibly the most common cause in young adults. Pleural effusions are common in both non-Hodgkin and Hodgkin lymphoma. In patients with non-Hodgkin lymphoma, approximately 16% will develop malignant effusions, and most will have the effusion at the time of initial diagnosis in association with evidence of disease elsewhere.
- 108. In some patients with non-Hodgkin lymphoma, chylothorax may also develop in one analysis of 88 patients with chylothorax, 12.5% were due to lymphoma, all non-Hodgkin lymphoma. In Hodgkin lymphoma, effusions may be caused by hilar or mediastinal lymph node involvement as well as pleural involvement. In one study of 110 patients presenting with Hodgkin lymphoma, effusions were present in 26 (24%); these were equally unilateral or bilateral. The presence of effusion was more common in those with higher-stage disease, extranodal involvement, and bulky mediastinal disease
- 109. Malignant mesothelioma is usually a unilateral disease ; bilateral tumors are present in less than 10% of patients. An early manifestation of the tumor is a pleural effusion that is reabsorbed or organized and then largely replaced by tumor and fibrosis. The tumor seldom penetrates deeply into the lung parenchyma; instead, it extends into interlobar fissures. Hilar lymph nodes are involved by tumor in less than 50% of patients. Distant hematogenous metastases are unusual but have been described in liver, bone, adrenals, thyroid, and kidneys.
- 110. Pathophysiology Lymph node / lymphatic spread breast and lung cancer Hematogenous spread lung cancer Lymphatic obstruction like hodgkin & nonhodgkin lymphoma Direct invasion of pleura like non hodgkin lymphoma and lung cancer Tumour invasion of blood vessels /haemorhagic pleural effusion like in breast cancer
- 111. Paramalignant PE Paramalignant effusions are pleural effusions found in patients with tumors without direct pleural involvement and no evidence of malignant cells in pleural fluid. Obstruction of the thoracic duct . Bronchial obstruction. Trapped lung. Chemotherapy (bleomycine,cyclophosphomide ,MTX) Radiation therapy Post obstructive pneumonia Pulmonary emboli
- 112. Prognosis MPE The overall prognosis is poor for most patients with malignant pleural effusions several studies with a total of over 400 patients, the median survival was 4.0months. The survival varied by tumor of origin; MPE from lung cancer had a median survival of 3.0 months MPE from cancer of the breast had 5.0 months MPE from mesothelioma 6.0 months, and from lymphoma 9.0 months.;
- 113. One of the strongest predictors appears to be the Karnofsky performance scale The Karnofsky Performance Score (KPS) ranking runs from 100 to 0, where 100 is "perfect" health and 0 is death.
- 115. in a prospective trial of 85 consecutive patients with malignant pleural effusions referred for thoracoscopic pleurodesis, those with a Karnofsky score above 70 had a median survival of 13.2 months, whereas those with a score below 30 had a median survival of 1.1 months.Interestingly, in this study, when compared to other measures such as pleural fluid pH, glucose level, or extent of carcinomatous involvement of the pleural surface, performance scoring was the only significant predictor of survival.
- 116. The life expectancy of patients with lung cancer and malignant pleural effusion has affected the revised staging classification of malignant pleural effusions In the 6TH edition of the TNM classification, effective since 1997, malignancy of the pleural space was considered a T4 lesion,and patients were staged as IIIB. However, in a comprehensive reassessment of staging and its effect on survival, patients with malignant pleural effusions were found to have a poorer prognosis than other T4M0 patients (8 months versus 13 months) and to be more similar to patients with metastatic disease to the other lung (10 months). In the revised staging system, pleural malignancy (malignant effusions or pleural nodular malignancy) is considered along with contralateral lung nodules as intrathoracic metastatic disease (M1a). Intrathoracic metastatic disease (M1a) is classified separately from extrathoracic metastatic disease (M1b) because of a somewhat better prognosis
- 117. Mangment Goal Survial? Palliation of symptom ? like dyspnea 90% Cough Chest discomfort The overall goal is to provide the greatest relief of symptoms using the least invasive, least morbid, and least expensive therapy
- 118. Repeated thoracentesis Immediate relief of symptom Higher recurrence rate Formation of adhesion Limit futures thoracoscopic intervention Limited survival <3 month
- 119. Management options Observation? Symptomatic controle Chemoresponsive tumorChemotherapy Slowly recurring effusion Used for patients with very short life expectancyThoracentesis Lung able to reinflate Can free up lung tacked down by adhesions, obtain biopsies Thoracoscopy must be available Pleurodesis Via chest tube Via thoracoscopy Survival >3 Good outpatient situation Good for trapped lungIndwelling tunneled catheter Patient able to operate pump Good for trapped lung Excellent for chylothoraxPleuroperitoneal shunt When other less invasive options have failedPleurectomy Via thoracoscopy Good patient status and life expectancyPleurectomy Via thoracotomy
- 120. cancers sensitive to chemotherapy like breast, sclc , and lymphoma Pleurodesis with talc is successful in most (70% to 100%) cases and is more effective than pleurodesis with other agents, including tetracycline and bleomycin
- 122. 56-y woman left sided chest pain beginning 1 week prior. The pain is described as severe, constant, and associated with dyspnea. No S&S of infection. She has been a smoker since the age of 18 no hx of tuberculosis. examination / vital S & spo2 normal ,diminished breath sounds over LFT chest with dullness to percussion and reduced tactile fremitus. CXR near-total opacication of the left hemithorax with slight contralateral displacement of the mediastinum. Bedside pleural ultrasonography confirms the presence of an effusion.
- 123. ResultParameter 7.43pH 4.7 g/dLtotal protein 1,068 U/LLactate dehydrogenase (LDH) 46% lymphocytes, 20% mesothelial cells Differential cell count +ve for malign.cell, favouring AD, pending immunhistochemicalstain Pleural fluid cytology
- 124. Question 1: Which one of the following clinical features of this case is most supportive of the diagnosis of malignant pleural mesothelioma (MPM) over lung adenocarcinoma? A. Pleural fluid LDH > 1,000 U/L B. Lack of asbestos exposure history C. History of smoking D. Severe constant chest pain E. Duration of symptoms
- 125. D. Severe constant chest pain Unlike lung AD, MPM does not have an established causal relationship with cigarette smoking. MPM patients tend to become symptomatic insidiously and it is there fore typical for them to present after months of symptoms; this patient’s presentation after one week of symptoms would be more consistent with a rapidly accumulating pleural effusion from adenocarcinoma. The chest pain that occurs with MPM classically becomes very severe and, unlike the pleuritic chest pain from metastatic pleural malignancy, is often described as constant. In both malignancies, the pleural fluid is a lymphocyte-predominant exudate capable of exhibiting LDH levels of > 1,000 U/L.
- 126. Question 2: Positivity for which of the following additional immunohistochemical markers beside calretinine would Favor the diagnosis of MPM over lung adenocarcinoma? A. WT -1 B. THyroid transcription Factor 1 (TTF-1) C. Napsin A D. Carcinoembryonic antigen (CEA) E. P63
- 127. Question 2: Positivity for which of the following additional immunohistochemical markers beside calretinine would Favor the diagnosis of MPM over lung adenocarcinoma? A. WT -1 B. THyroid transcription Factor 1 (TTF-1) are specific markers for AD C. Napsin A D. Carcinoembryonic antigen (CEA) E. P63 is specific for squamous cell carcinoma
- 128. Which of the following is true about the diagnosis of MPM? A. Surgical pleural biopsy does not increase diagnostic yield over guided cutting needle biopsy. B. The serum biomarkers megakaryocyte potentiation factor (MPF) and osteopontin exhibit sensitivities of < 50% for MPM. C. Finding sarcomatoid histology in a patient with MPM is a favorable prognostic indicator. D. The TNM staging system cannot be applied to the prognostication o MPM. E. Male gender portends a favorable prognosis in MPM.
- 129. A. Surgical pleural biopsy does not increase diagnostic yield over guided cutting needle biopsy. guided needle biopsy of the pleura in MPM is far inferior to that of surgical pleural biopsy. (VATS) is the optimal diagnostic modality for MPM and also allows for easier histologic subtyping into the epithelioid, sarcomatoid, and mixed variants, which has prognostic and treatment implications B. The serum biomarkers megakaryocyte potentiation factor (MPF) and osteopontin exhibit sensitivities of < 50% for MPM. C. Finding sarcomatoid histology in a patient with MPM is a favorable prognostic indicator. D. The TNM staging system cannot be applied to the prognostication o MPM.TNM and other staging are applied E. Male gender portends a favorable prognosis in MPM.
- 130. 75 y old retired builder, 2-month history of SOB on exertion with associated chest pain, which he describes as a dull discomfort. NO PMHX no HX of regular medications. Up until his symptoms developed he was independent with all his activities of daily living. O/E decreased breath sounds on the right hand side CXR right-sided pleural effusion with pleural thickening. the patient was referred to surgical (VATS) biopsy to confirm the diagnosis.
- 131. What is the most appropriate management? Chemotherapy Chest drain insertion Pneumonectomy Radical radiotherapy Radiotherapy to surgical port sites
- 132. What is the most appropriate management? Chemotherapy Chest drain insertion Pneumonectomy Radical radiotherapy Radiotherapy to surgical port sites
- 133. Patients with good performance status could be considered for palliative chemotherapy, which can result in tumour shrinkage. Palliative radiotherapy can be useful to reduce chest pain, shortness of breath and to relieve superior vena cava obstruction but would not be appropriate in our patient at present. There is no evidence of benefit for radiology at the surgical port sites and surgical resection remains controversial. Chest drains are usually reserved for recurrent pleural effusions and those that fail talc pleurodesis.